Hip fractures are an important topic in trauma and orthopaedics. They are common and lead to significant morbidity and mortality. The 30-day mortality is 5-10%. Half of patients become less independent after a hip fracture.
Increasing age and osteoporosis are major risk factors for hip fractures. Females are affected more often than males.
Due to the morbidity and mortality with hip fractures, they are generally prioritised on the trauma list with the aim to perform surgery within 48 hours. There is also a specialty called orthogeriatrics, who focus on identifying and optimising the medical co-morbidities and complications of inpatients on the orthopaedic ward, particularly elderly patients with hip fractures.
Hip fractures can be categorised into:
- Intra-capsular fractures
- Extra-capsular fractures
Basic Anatomy
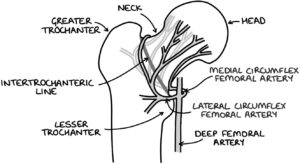
There are some basic structures of the top of the femur:
- Head
- Neck
- Greater trochanter (lateral)
- Lesser trochanter (medial)
- Intertrochanteric line
- Shaft (body)
The capsule of the hip joint is a strong fibrous structure. It attaches to the rim of the acetabulum on the pelvis and the intertrochanteric line on the femur. It surrounds the neck and head of the femur.
The head of the femur has a retrograde blood supply. The medial and lateral circumflex femoral arteries join the femoral neck just proximal to the intertrochanteric line. Branches of this artery run along the surface of the femoral neck, within the capsule, towards the femoral head. They provide the only blood supply to the femoral head. A fracture of the intra-capsular neck of the femur can damage these blood vessels, removing the blood supply to the femoral head, leading to avascular necrosis. Therefore, patients with a displaced intra-capsular fracture need to have the femoral head replaced with a hemiarthroplasty or total hip replacement.
TOM TIP: It is worth understanding and remembering the concept of the retrograde blood supply to the head of the femur and how this determines the choice of operation (explained below). When I did an FY1 job in trauma and orthopaedics, the juniors were questioned on this concept almost every time a patient with a hip fracture was admitted. Being able to identify the type of hip fracture on an x-ray (intra-capsular or extra-capsular) and justify the choice of operation made trauma meetings much less stressful.
Intra-Capsular Fractures
Intra-capsular fractures involve a break in the femoral neck, within the capsule of the hip joint. This affects the area proximal to the intertrochanteric line.
The Garden classification is used for intra-capsular neck of femur fractures:
- Grade I – incomplete fracture and non-displaced
- Grade II – complete fracture and non-displaced
- Grade III – partial displacement (trabeculae are at an angle)
- Grade IV – full displacement (trabeculae are parallel)
Non-displaced intra-capsular fractures may have an intact blood supply to the femoral head, meaning it may be possible to preserve the femoral health without avascular necrosis occurring. They can be treated with internal fixation (e.g., with screws) to hold the femoral head in place while the fracture heals.
Displaced intra-capsular fractures (grade III and IV) disrupt the blood supply to the head of the femur. Therefore, the head of the femur needs to be removed and replaced.
Hemiarthroplasty involves replacing the head of the femur but leaving the acetabulum (socket) in place. Cement is used to hold the stem of the prosthesis in the shaft of the femur. This is generally offered to patients who have limited mobility or significant co-morbidities.
Total hip replacement involves replacing both the head of the femur and the socket. This is generally offered to patients who can walk independently and are fit for surgery.
Extra-Capsular Fractures
Extra-capsular fractures leave the blood supply to the head of the femur intact. Therefore, the head of the femur does not need to be replaced.
Intertrochanteric fractures occur between the greater and lesser trochanter. These are treated with a dynamic hip screw (AKA sliding hip screw). A screw goes through the neck and into the head of the femur. A plate with a barrel that holds the screw is screwed to the outside of the femoral shaft. The screw that goes through the femur to the head allows some controlled compression at the fracture site, whilst still holding it in the correct alignment. Adding some controlled compression across the fracture improves healing.
Subtrochanteric fractures occur distal to the lesser trochanter (although within 5cm). The fracture occurs to the proximal shaft of the femur. These may be treated with an intramedullary nail (a metal pole inserted through the greater trochanter into the central cavity of the shaft of the femur).
Hip Fracture Presentation
The typical scenario is an older patient (over 60) who has fallen, presenting with:
- Pain in the groin or hip, which may radiate to the knee
- Not able to weight bear
- Shortened, abducted and externally rotated leg
An essential part of assessing patients with a new hip fracture is to determine any other acute illnesses. There is often a good reason for them to fall and break a hip. They may also be suffering with:
- Anaemia
- Electrolyte imbalances
- Arrhythmias
- Heart failure
- Myocardial infarction
- Stroke
- Urinary or chest infection
These conditions need to be identified as early as possible so that the patient can be optimised and surgery can proceed with minimal delays.
TOM TIP: The term “mechanical fall” is often used to imply a simple explanation for why the patient fell, such as tripping over an object or being knocked over. It is worth exploring the fall in more detail. In many cases, there may be a correctable underlying medical cause for the fall, such as anaemia, arrhythmia or even underlying Parkinson’s disease. There may also be social contributors to the fall, such as dehydration, incorrect eyewear, poor footwear or obstacles in the home. If you identify an underlying reversible cause, you could make a big difference to that patient and impress your orthogeriatric colleagues.
Imaging
X-rays are the initial investigation of choice. Two views are essential, as a single view can miss the fracture. Anterior-to-posterior (AP) and lateral views are standard.
Shenton’s line can be seen on an AP x-ray of the hip. It is one continuous curving line formed by the medial border of the femoral neck and continues to the inferior border of the superior pubic ramus. Disruption of Shenton’s line is a key sign of a fractured neck of femur (NOF).
MRI or CT scanning may be used where the x-ray is negative, but a fracture is still suspected.
Management
On admission, patients will have:
- Appropriate analgesia
- Investigations to establish the diagnosis (e.g., x-rays)
- Venous thromboembolism risk assessment and prophylaxis (e.g., low molecular weight heparin)
- Pre-operative assessment (including bloods and an ECG) to ensure they are fit and optimised for surgery
- Orthogeriatrics input
The NICE guidelines (updated 2017) say that surgery should be carried out either the same day or the day after the patient is admitted (within 48 hours).
The operation should allow the patient to weight bear straight away. This allows the physiotherapists to start mobilisation and rehabilitation as soon as possible after the operation. Post-operative analgesia is important to encourage the patient to mobilise as quickly as possible.
Last updated August 2021
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()