Volvulus is a condition where the bowel twists around itself and the mesentery that it is attached to. The mesentery is the membranous peritoneal tissue that creates a connection between the bowel and the posterior abdominal wall. The bowel gets its blood supply from the mesentery (through the mesenteric arteries).
Twisting in the bowel leads to a closed-loop bowel obstruction, where a section of bowel is isolated by obstruction on either side.
The blood vessels that supply the bowel can be involved, cutting off the blood supply to the bowel, which leads to bowel ischaemia. Ischaemia leads to death of the bowel tissue (necrosis), and bowel perforation.
Types of Volvulus
There are two main types of volvulus depending on the area affected:
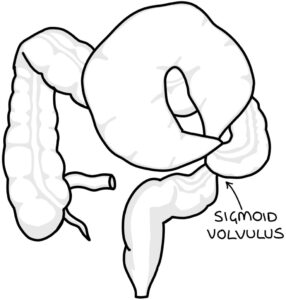
- Sigmoid volvulus
- Caecal volvulus
Sigmoid volvulus is more common and tends to affect older patients. The twist affects the sigmoid colon. A key cause is chronic constipation and lengthening of the mesentery attached to the sigmoid colon. The sigmoid colon becomes overloaded with faeces, causing it to sink downwards causing a twist. It is also associated with a high fibre diet and the excessive use of laxatives.
Caecal volvulus is less common and tends to affect younger patients. The twist occurs in the caecum.
Risk Factors
- Neuropsychiatric disorders (e.g., Parkinson’s)
- Nursing home residents
- Chronic constipation
- High fibre diet
- Pregnancy
- Adhesions
Presentation
The signs and symptoms are akin to bowel obstruction, with:
- Vomiting (particularly green bilious vomiting)
- Abdominal distention
- Diffuse abdominal pain
- Absolute constipation and lack of flatulence
Diagnosis
Abdominal x-ray can show the “coffee bean” sign in sigmoid volvulus, where the dilated and twisted sigmoid colon looks like a giant coffee bean.
A contrast CT scan is the investigation of choice to confirm the diagnosis and identify other pathology.
TOM TIP: Remember the “coffee bean” sign for your MCQ exams. It is worth looking up photographs so that you can recognise it and immediately know the diagnosis (sigmoid volvulus) if it comes up.
Management
The initial management is the same as with bowel obstruction (nil by mouth, NG tube and IV fluids).
Conservative management with endoscopic decompression can be attempted in patients with sigmoid volvulus (without peritonitis). A flexible sigmoidoscope is inserted carefully, with the patient in the left lateral position, resulting in a correction of the volvulus. A flatus tube / rectal tube is left in place temporarily to help decompress the bowel and is later removed. There is a risk of recurrence (around 60%).
Surgical management involves:
- Laparotomy (open abdominal surgery)
- Hartmann’s procedure for sigmoid volvulus (removal of the rectosigmoid colon and formation of a colostomy)
- Ileocaecal resection or right hemicolectomy for caecal volvulus
Last updated May 2021
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()