A bowel obstruction refers to when the passage of food, fluids and gas, through the intestines becomes blocked. Small bowel obstruction is more common than large bowel obstruction. Obstruction results in a build up of gas and faecal matter proximal to the obstruction (before the obstruction). This causes back-pressure, resulting in vomiting and dilatation of the intestines proximal to the obstruction. Bowel obstruction is a surgical emergency.
The gastrointestinal tract secretes fluid that is later absorbed in the colon. When there is an obstruction, and fluid cannot reach the colon, it cannot be reabsorbed. As a result, there is fluid loss from the intravascular space into the gastrointestinal tract. This leads to hypovolaemia and shock. This abnormal loss of fluid is referred to as third-spacing. The higher up the intestine the obstruction, the greater the fluid losses as there is less bowel over which the fluid can be reabsorbed.
Causes
The “big three” causes account for around 90% of cases:
- Adhesions (small bowel)
- Hernias (small bowel)
- Malignancy (large bowel)
Other causes include:
- Volvulus (large bowel)
- Diverticular disease
- Strictures (e.g., secondary to Crohn’s disease)
- Intussusception (in young children aged 6 months to 2 years)
TOM TIP: Learn to recite the “big three” causes of obstruction without any hesitation. These are the three causes of bowel obstruction you should produce if asked on a ward round or in an OSCE examination. When patients present with symptoms of bowel obstruction, don’t just think about obstruction, but also consider what the cause of the obstruction would be. Ask about hernias, change in bowel habit, weight loss and PR bleeding (bowel cancer) and about previous abdominal surgery that may have resulted in adhesions.
Adhesions
Adhesions are pieces of scar tissue that bind the abdominal contents together. They can cause kinking or squeezing of the bowel, leading to obstruction. Adhesions typically cause obstruction in the small bowel, rather than the large bowel.
The main causes of intestinal adhesions are:
- Abdominal or pelvic surgery (particularly open surgery)
- Peritonitis
- Abdominal or pelvic infections (e.g., pelvic inflammatory disease)
- Endometriosis
Less commonly, they can be congenital or secondary to radiotherapy treatment.
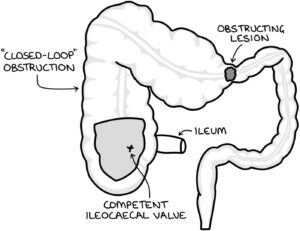
Closed-Loop Obstruction
Closed-loop obstruction describes a situation where there are two points of obstruction along the bowel; meaning that there is a middle section sandwiched between two points of obstruction. This might happen with:
- Adhesions that compress two areas of bowel
- Hernias that isolate a section of bowel blocking either end
- Volvulus where the twist isolates a section of intestine
- A single point of obstruction in the large bowel, with an ileocaecal valve that is competent
A competent ileocaecal valve does not allow any movement back into the ileum from the caecum. When there is a large bowel obstruction and a competent ileocaecal valve, a section of bowel becomes isolated and the contents cannot flow in either direction.
The contents of a “closed-loop” section of bowel do not have an open end where they can drain and decompress. Therefore, the closed-loop section will inevitably continue to expand, leading to ischaemia and perforation. Closed-loop obstruction requires emergency surgery.
Presentation
The key features of bowel obstruction are:
- Vomiting (particularly green bilious vomiting)
- Abdominal distention
- Diffuse abdominal pain
- Absolute constipation and lack of flatulence
- “Tinkling” bowel sounds may be heard in early bowel obstruction
Abdominal X-ray
The key x-ray finding in bowel obstruction is distended loops of bowel.
The upper limits of the normal diameter of bowel are:
- 3 cm small bowel
- 6 cm colon
- 9 cm caecum
Valvulae conniventes are present in the small bowel and are mucosal folds that form lines extending the full width of the bowel. These are seen on an abdominal x-ray as lines across the entire width of the bowel.
Haustra are like pouches formed by the muscles in the walls of the large bowel. They form lines that do not extend the full width of the bowel. These are seen on an abdominal x-ray as lines that extend only part of the way across the bowel.
Initial Management
As with any unwell patient, start with an ABCDE approach. Patients with bowel obstruction may be haemodynamically unstable and require urgent intervention if they have developed:
- Hypovolaemic shock due to fluid stuck in the bowel rather than the intravascular space (third-spacing)
- Bowel ischaemia
- Bowel perforation
- Sepsis
A full set of bloods are required, as with any acute abdomen. Key things to look out for with bowel obstruction are:
- Electrolyte imbalances (U&Es)
- Metabolic alkalosis due to vomiting stomach acid (venous blood gas)
- Bowel ischaemia (raised lactate – either on a venous blood gas or laboratory sample)
The initial management of bowel obstruction is casually described as “drip and suck”:
- Nil by mouth (don’t put food or fluids in if there is a blockage)
- IV fluids to hydrate the patient and correct electrolyte imbalances
- NG tube with free drainage to allow stomach contents to freely drain and reduce the risk of vomiting and aspiration
Abdominal x-ray may be the initial imaging investigation. However, depending on the signs and symptoms, this may be skipped, and the patient sent straight for a CT scan.
Erect chest x-ray can demonstrate air under the diaphragm when there is an intra-abdominal perforation.
A contrast abdominal CT scan is usually required to confirm the diagnosis of bowel obstruction and establish the site and cause of the obstruction. It can also be used to diagnose an intra-abdominal perforation, if present.
Surgical Intervention
Conservative management may be used in the first instance in stable patients with obstruction secondary to adhesions or volvulus. Where this fails, surgery is required.
The definitive management of bowel obstruction is with surgery (either laparoscopy or laparotomy) to correct the underlying cause:
- Exploratory surgery in patients with an unclear underlying cause
- Adhesiolysis to treat adhesions
- Hernia repair
- Emergency resection of the obstructing tumour
Stents may be inserted into the bowel (during a colonoscopy) in patients with obstruction due to a tumour. Stents hold the tumour out of the way, creating space for the bowel contents to move through.
Last updated May 2021
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()