Haemorrhoids are enlarged anal vascular cushions. It is not clear why they become enlarged and swollen, but they are often associated with constipation and straining. They are also more common with pregnancy, obesity, increased age and increased intra-abdominal pressure (e.g., weightlifting or chronic coughing).
They often occur in pregnancy, most likely due to constipation, pressure from the baby in the pelvis and the effects of hormones that relax the connective tissues.
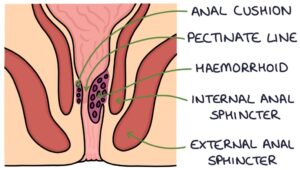
Anal Cushions
The anal cushions are specialised submucosal tissue that contain connections between the arteries and veins, making them very vascular. They are supported by smooth muscle and connective tissue. They help to control anal continence, along with the internal and external sphincters. The blood supply is from the rectal arteries.
The location of pathology at the anus is described as a clock face, as though the patient was in the lithotomy position (on their back with their legs raised). 12 o’clock is towards the genitals and 6 o’clock is towards the back. The anal cushions are usually located at 3, 7 and 11 o’clock.
Classification
The classification of haemorrhoids depends on their size and whether they prolapse from the anus:
- 1st degree: no prolapse
- 2nd degree: prolapse when straining and return on relaxing
- 3rd degree: prolapse when straining, do not return on relaxing, but can be pushed back
- 4th degree: prolapsed permanently
Symptoms
Haemorrhoids may be asymptomatic. They are often associated with constipation and straining.
A common presentation is with painless, bright red bleeding, typically on the toilet tissue or seen after opening the bowels. The blood is not mixed with the stool (this should make you think of an alternative diagnosis).
Other symptoms include:
- Sore / itchy anus
- Feeling a lump around or inside the anus
Examination
- External (prolapsed) haemorrhoids are visible on inspection as swellings covered in mucosa
- Internal haemorrhoids may be felt on a PR exam (although this is generally difficult or not possible)
- They may appear (prolapse) if the patient is asked to “bear down” during inspection
Proctoscopy is required for proper visualisation and inspection. This involves inserting a hollow tube (proctoscope) into the anal cavity to visualise the mucosa.
Management
Consider the differential diagnoses in patients presenting with symptoms such as rectal bleeding:
- Anal fissures
- Diverticulosis
- Inflammatory bowel disease
- Colorectal cancer
Consider testing for anaemia if there is prolonged bleeding or clinical signs of anaemia.
Topical treatments can be given for symptomatic relief and to help reduce swelling, for example:
- Anusol (contains chemicals to shrink the haemorrhoids – “astringents”)
- Anusol HC (also contains hydrocortisone – only used short term)
- Germoloids cream (contains lidocaine – a local anaesthetic)
- Proctosedyl ointment (contains cinchocaine and hydrocortisone – short term only)
Prevention and treatment of constipation involves:
- Increasing the amount of fibre in the diet
- Maintaining a good fluid intake
- Using laxatives where required
- Consciously avoiding straining when opening their bowels
There are a number of non-surgical treatments for haemorrhoids:
- Rubber band ligation (fitting a tight rubber band around the base of the haemorrhoid to cut off the blood supply)
- Injection sclerotherapy (injection of phenol oil into the haemorrhoid to cause sclerosis and atrophy)
- Infra-red coagulation (infra-red light is applied to damage the blood supply)
- Bipolar diathermy (electrical current applied directly to the haemorrhoid to destroy it)
Surgical Options
Haemorrhoidal artery ligation involves using a proctoscope to identify the blood vessel that supplies the haemorrhoids and suturing it to cut off the blood supply.
Haemorrhoidectomy involves excising the haemorrhoid. Removing the anal cushions may result in faecal incontinence.
Stapled haemorrhoidectomy involves using a special device that excises a ring of haemorrhoid tissue at the same time as adding a circle of staples in the anal canal. The staples remain in place long-term.
Thrombosed Haemorrhoids
Thrombosed haemorrhoids are caused by strangulation at the base of the haemorrhoid, resulting in thrombosis (a clot) in the haemorrhoid. This can be very painful.
Thrombosed haemorrhoids appear as purplish, very tender, swollen lumps around the anus. A PR examination is unlikely to be possible due to the pain.
They will resolve with time, although this can take several weeks.
The NICE Clinical Knowledge Summaries (2016) suggests considering admission if the patient present within 72 hours with extremely painful thrombosed haemorrhoids. They may benefit from surgical management.
Last updated May 2021
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()