Severe pathology of the aortic or mitral valves may be an indication for surgical replacement of that valve. Replacement of the tricuspid valve is very rare.
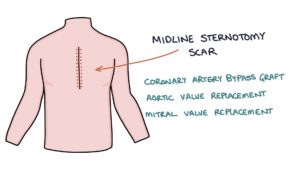
Patients that have had a valve replacement will have a scar. Usually, this will be a midline sternotomy scar straight down the middle of the sternum indicating a mitral or aortic valve replacement or a coronary artery bypass graft (CABG). Less commonly a right-sided mini-thoracotomy incision can be used for minimally invasive mitral valve surgery.
Aortic Stenosis
Severe aortic stenosis is the most common valvular heart disease you will encounter and the most common indication for valve replacement surgery.
Aortic stenosis causes an ejection-systolic, high-pitched murmur (high velocity of systole). This has a crescendo-decrescendo character due to the speed of blood flow across the value during the different periods of systole. Flow during systole is slowest at the very start and end, and is fastest in the middle.
Other signs:
- The murmur radiates to the carotids as the turbulence continues up into the neck
- Slow rising pulse and narrow pulse pressure
- Patients may complain of exertional syncope (lightheadedness and fainting when exercising) due to difficulty maintaining a good flow of blood to the brain
Causes:
- Idiopathic age-related calcification (by far the most common cause)
- Rheumatic heart disease
Mitral Regurgitation
Mitral regurgitation is the second most common indication for valve replacement.
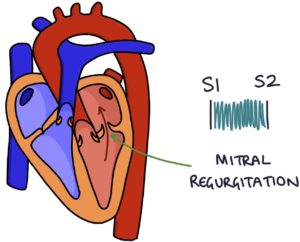
Mitral regurgitation is when an incompetent mitral valve allows blood to leak back through during systolic contraction of the left ventricle.
The leaking valve causes a reduced ejection fraction and a backlog of blood waiting to be pumped through the left side of the heart, resulting in congestive cardiac failure.
Mitral regurgitation causes a pan-systolic, high pitched “whistling” murmur due to high-velocity blood flow through the leaky valve. The murmur radiates to the left axilla. You may hear a third heart sound.
Causes:
- Idiopathic weakening of the valve with age
- Ischaemic heart disease
- Infective endocarditis
- Rheumatic heart disease
- Connective tissue disorders, such as Ehlers Danlos syndrome or Marfan syndrome
Bioprosthetic Versus Mechanical
Valves can be either replaced by a bioprosthetic or a metallic mechanical valve.
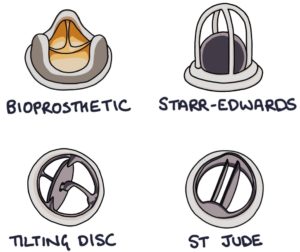
Bioprosthetic valves have a limited lifespan of around 10 years. “Porcine” bioprosthetic valves come from a pig.
Mechanical valves have a good lifespan (well over 20 years) but require lifelong anticoagulation with warfarin. The INR target range with mechanical valves is 2.5 – 3.5 (this is higher than the 2 – 3 target for atrial fibrillation).
Types of Mechanical Heart Valves
Starr-Edwards valve features a ball in a cage. The ball moves away from the opening to let blood through, then moves back against the opening to prevent blood from regurgitating through the valve. They were very successful but are no longer used due to the high risk of thrombus formation.
Tilting disc valves feature a single tilting disc.
A St Jude valve consists of two tilting metal discs. The two discs mean they are called bileaflet valves. Of the three mechanical valves listed, the St Jude valve has the smallest risk of thrombus formation.
Mechanical Heart Valves
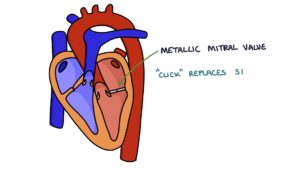
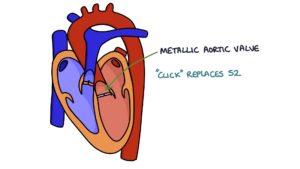
It is possible to hear a click when auscultating the heart sounds in a patient with a mechanical valve:
- A click replaces S1 for metallic mitral valve
- A click replaces S2 for metallic aortic valve
There are three major complications of mechanical heart valves:
- Thrombus formation (blood stagnates and clots)
- Infective endocarditis (infection in prosthesis)
- Haemolysis causing anaemia (blood gets churned up in the valve)
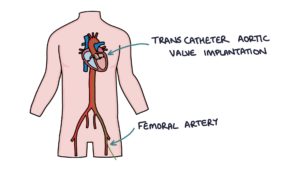
Transcatheter Aortic Valve Implantation (TAVI)
This is a treatment for severe aortic stenosis, usually in patients that are at high risk for an open valve replacement operation. It involves local or general anaesthetic, inserting a catheter into the femoral artery, feeding a wire under x-ray guidance to the location of the aortic valve, then inflating a balloon to stretch the stenosed aortic valve and implanting a bioprosthetic valve in the location of the aortic valve.
Long term outcomes for TAVI are still not clear as it is a relatively new procedure. Therefore, in younger, fitter patients, open surgery is still the first-line option.
Patients that have a TAVI do not typically require warfarin as the valve is bioprosthetic.
Infective Endocarditis
This occurs in around 2.5% of patients having a surgical valve replacement. The rate is slightly lower for TAVI at around 1.5%. Infective endocarditis in a prosthetic valve has quite a high mortality of around 15%. This is usually caused by one of three gram-positive cocci organisms:
- Staphylococcus
- Streptococcus
- Enterococcus
Last updated May 2021
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()