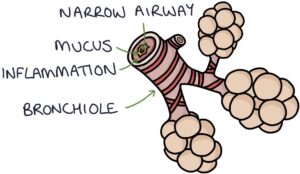
Bronchiolitis involves infection and inflammation in the bronchioles, the small airways of the lungs. It occurs most commonly in the winter months.
Respiratory syncytial virus (RSV) is the most common cause. Other causes include rhinovirus and adenovirus.
Bronchiolitis is generally considered to occur in infants under 1 year. It is most common in infants under 6 months. It can be diagnosed in children up to 2 years of age, particularly in ex-premature babies with chronic lung disease.
Infants with bronchiolitis are more likely to develop viral-induced wheeze or asthma during childhood.
Basic Pathophysiology
Inflammation, oedema, and increased mucus production in the bronchioles cause the airway to narrow, obstructing the flow of air. Infants’ airways are very small, so even minimal narrowing can cause significant symptoms. Airflow obstruction causes increased work of breathing and reduced oxygen saturation.
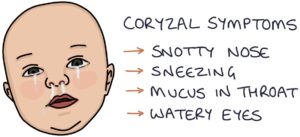
Respiratory syncytial virus (RSV) infection usually starts with coryzal symptoms (runny nose, sneezing and a sore throat).
Around half of infants with RSV infection go on to develop bronchiolitis. A typical course of illness involves:
- Chest symptoms 1-2 days after the onset of coryzal symptoms
- Peak of symptoms on days 3-5
- Symptoms lasting 7-10 days total
- Full recovery within 3 weeks
Presentation
Presenting symptoms include:
- Coryzal symptoms (runny nose, sneezing, watery eyes)
- Dyspnoea (heavy laboured breathing)
- Tachypnoea (fast breathing)
- Reduced feeding
- Mild fever (under 39ºC)
- Apnoeas (episodes where the child stops breathing)
- Cyanosis (due to low oxygen saturation)
Auscultation findings include widespread harsh breath sounds, wheezes and crackles.
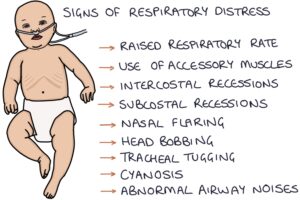
Signs of respiratory distress include:
- Raised respiratory rate
- Accessory muscle use (e.g., sternocleidomastoid, abdominal and intercostal muscle use)
- Intercostal and subcostal recessions
- Nasal flaring
- Head bobbing
- Tracheal tug
- Grunting
TOM TIP: You should become very confident in listing and spotting the signs of respiratory distress. This is very important when assessing children with respiratory illnesses.
Abnormal Airway Noises
Wheezing is a whistling sound heard on auscultation and caused by airway obstruction. It occurs during exhalation. Widespread wheeze may be heard in children with bronchiolitis, asthma, and viral-induced wheeze. A focal wheeze suggests a localised condition, such as foreign body aspiration or an obstructing tumour.
Grunting is caused by exhaling with the glottis partially closed to create positive end-expiratory pressure. It helps keep air in the airways, stopping them from collapsing during exhalation. It can be a sign of significant respiratory illness.
Stridor is a high-pitched inspiratory noise caused by obstruction of the upper airway. It is not typically a feature of bronchiolitis. Causes of stridor include:
- Foreign body aspiration
- Croup
- Epiglottitis
- Laryngomalacia
Admission
Most infants can be managed at home with advice about when to seek further medical attention.
Reasons for admission include:
- Aged under 3 months
- Pre-existing condition (e.g., prematurity, congenital heart disease, cystic fibrosis or Down’s syndrome)
- Less than 50-75% of their normal fluid intake
- Signs of dehydration (e.g., reduced urine output, dry mucus membranes or reduced skin turgor)
- Respiratory rate above 70
- Oxygen saturation below 92%
- Persistent severe signs of respiratory distress (e.g., deep recessions or grunting)
- Apnoeas
- Cyanosis
- Difficulty managing or seeking medical help from home
Management
Management of bronchiolitis involves:
- Ensuring adequate intake (oral, NG feeds or IV fluids depending on the severity)
- Saline nasal drops and nasal suctioning may help clear nasal secretions, particularly before feeding
- Supplementary oxygen if the oxygen saturations remain below 90% (or 92% if under 6 weeks or high risk)
- Ventilatory support, if required
A full stomach restricts breathing. Smaller and more frequent feeds may be better tolerated.
The guidelines recommend against nebulised hypertonic saline, bronchodilators, steroids and antibiotics.
Respiratory Support
Respiratory support may be required in severe bronchiolitis. These can be stepped up as required:
- Low-flow oxygen (e.g., 2 litres via nasal cannula)
- High-flow humidified oxygen via a tight nasal cannula (e.g., “Airvo” or “Optiflow”)
- Continuous positive airway pressure (CPAP)
- Intubation and ventilation
High-flow humidified oxygen adds positive end-expiratory pressure (PEEP) to help maintain the airways and prevent them from collapsing during exhalation.
CPAP involves using a sealed nasal cannula to deliver greater positive end-expiratory pressure (PEEP).
Intubation and ventilation involve inserting an endotracheal tube into the trachea and fully controlling breathing using mechanical ventilation.

Capillary blood gases may be used to monitor the response to treatment in severe bronchiolitis requiring significant respiratory support. Signs of inadequate ventilation include:
- Rising pCO2 (severe airway obstruction reduces the clearance of carbon dioxide)
- Falling pH (rising carbon dioxide causes respiratory acidosis)

Respiratory Syncytial Virus Vaccine
The RSV vaccine is recommended for all pregnant women from 28 weeks of gestation. It creates an immune response in the mother, generating antibodies that pass through the placenta to the fetus. These antibodies offer the baby protection for the first 6 months of life.
Palivizumab
Palivizumab is a monoclonal antibody that targets the respiratory syncytial virus. It involves monthly injections and is given to high-risk babies, such as ex-premature and those with congenital heart disease.
Palivizumab provides passive protection against RSV. Antibodies against RSV are injected, and the immune system does not create any new antibodies (unlike vaccines). The antibody levels decrease over time, and repeated doses are required to maintain protection.

Last updated January 2025
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()