Pyloric stenosis involves thickening (hypertrophy) and narrowing of the pylorus, which connects the stomach and the duodenum. This prevents food from passing from the stomach to the duodenum as normal.
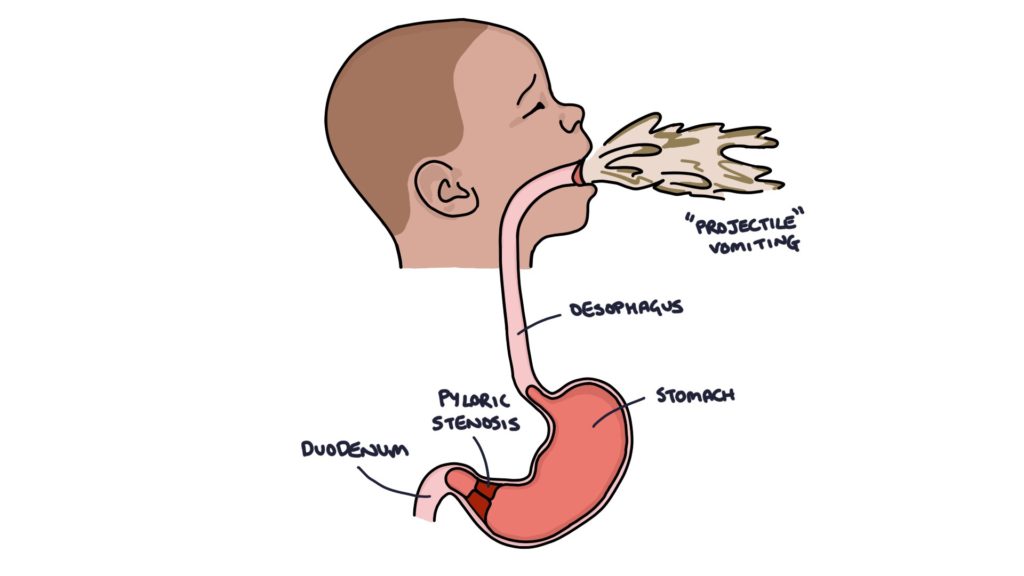
After feeding, increasingly powerful peristalsis of the stomach attempts to push food into the duodenum. Eventually, it becomes so powerful that the feed is ejected into the oesophagus, out of the mouth and across the room. This is called “projectile vomiting”.
Features
Pyloric stenosis typically presents before 3 months of age, with a hungry baby that is thin, pale and failing to thrive.
Forceful or “projectile” vomiting is the key presenting feature.
When examined after feeding, peristalsis may be seen on observation of the abdomen. A firm, round mass may be felt in the upper abdomen that feels “like a large olive”, caused by the hypertrophic pylorus.
Blood gas analysis shows a hypochloric (low chloride) metabolic alkalosis as the baby is vomiting the hydrochloric acid from the stomach.
Management
Diagnosis is made using an abdominal ultrasound to visualise the thickened pylorus.
Treatment is with a laparoscopic pyloromyotomy. An incision is made in the smooth muscle of the pylorus to widen the canal, widening the space for food to pass from the stomach to the duodenum.
The prognosis is good following the operation.
Last updated February 2025
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()