Tonsillitis refers to inflammation of the tonsils. It is most common in school-aged children and young adults.
Causes
The most common cause of an acute sore throat is a viral infection.
Group A streptococcus (Streptococcus pyogenes) is the key bacterial cause of acute tonsillitis.
Other important causes of acute sore throat in a child or young adult include:
- Infectious mononucleosis caused by Epstein-Barr virus (EBV)
- Group C and G streptococci
- Candidal pharyngitis (if immunocompromised, following antibiotics, or inhaled steroids)
- Diphtheria (rare in vaccinated children)
- Epiglottitis caused by Haemophilus influenzae type b (rare in vaccinated children)
Waldeyer’s Tonsillar Ring
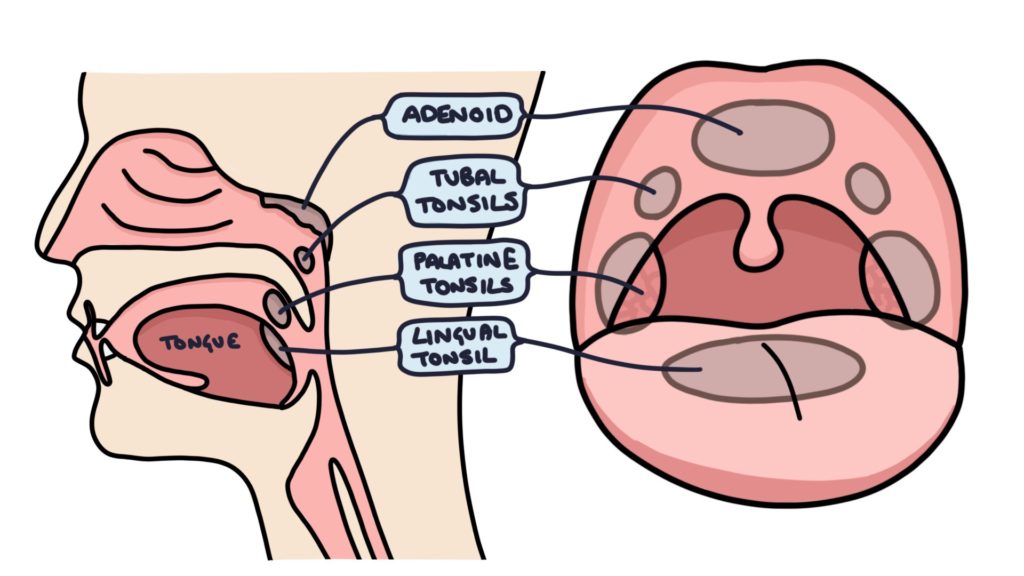
In the pharynx, at the back of the throat, there is a ring of lymphoid tissue. There are six areas of lymphoid tissue:
- Palatine tonsils (pair)
- Tubal tonsils (pair)
- Adenoids
- Lingual tonsil
The palatine tonsils are the ones typically infected and enlarged in tonsillitis.
Presentation
A typical presentation is a child with a fever, sore throat and painful swallowing.
Tonsillitis can present with non-specific symptoms, particularly in younger children. They may present only with a fever, poor oral intake, headache, vomiting or even abdominal pain.
Examination of the throat will reveal red, inflamed and enlarged tonsils, with or without exudates. Exudates are small white patches of pus on the tonsils.
Important additional steps when examining a child with tonsillitis include:
- Physical observations (including temperature, heart rate and respiratory rate) for systemic illness
- Otoscopy to assess for ear infection
- Neck palpation for cervical lymphadenopathy
Scoring Systems
The Centor criteria can be used to estimate the probability that tonsillitis is due to a bacterial infection, helping guide decision-making about antibiotics. A score of 3 or more indicates a 40-60% probability of bacterial tonsillitis. A point is given if each of the following features is present:
- Fever over 38ºC
- Tonsillar exudates
- Absence of cough
- Tender anterior cervical lymph nodes (lymphadenopathy)
The FeverPAIN score is an alternative to the Centor criteria. A score of 2-3 gives a 34-40% probability, and 4-5 gives a 62-65% probability of bacterial tonsillitis:
- Fever during the previous 24 hours
- P – Purulence (pus on tonsils)
- A – Attended within 3 days of the onset of symptoms
- I – Inflamed tonsils (severely inflamed)
- N – No cough or coryza
Management
Most cases are viral and can be managed with:
- Self-care (e.g., rest and fluid)
- Simple analgesia (e.g., paracetamol or ibuprofen)
- Safetynet advice (e.g., to return if not improving after 3 days or a fever above 38.3°C)
Antibiotics are considered when:
- Centor score is ≥ 3
- FeverPAIN score is ≥ 4
- Increased risk of serious infection (e.g., young infants or immunocompromised)
Delayed prescriptions can be considered. This involves educating patients or parents about the likely viral nature of the sore throat and issuing a prescription to be collected only if the symptoms do not improve or worsen over the next 2-3 days.
Penicillin V (phenoxymethylpenicillin) for 5-10 days is typically first-line. It has a relatively narrow spectrum of activity and is effective against Streptococcus pyogenes.
Clarithromycin is the usual first-line choice in true penicillin allergy.
Complications
Complications of tonsillitis include:
- Peritonsillar abscess, also known as quinsy
- Airway obstruction
- Otitis media, if the infection spreads via the Eustachian tube to the middle ear
- Scarlet fever
- Rheumatic fever
- Post-streptococcal glomerulonephritis
- Post-streptococcal reactive arthritis
Last updated May 2026
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()