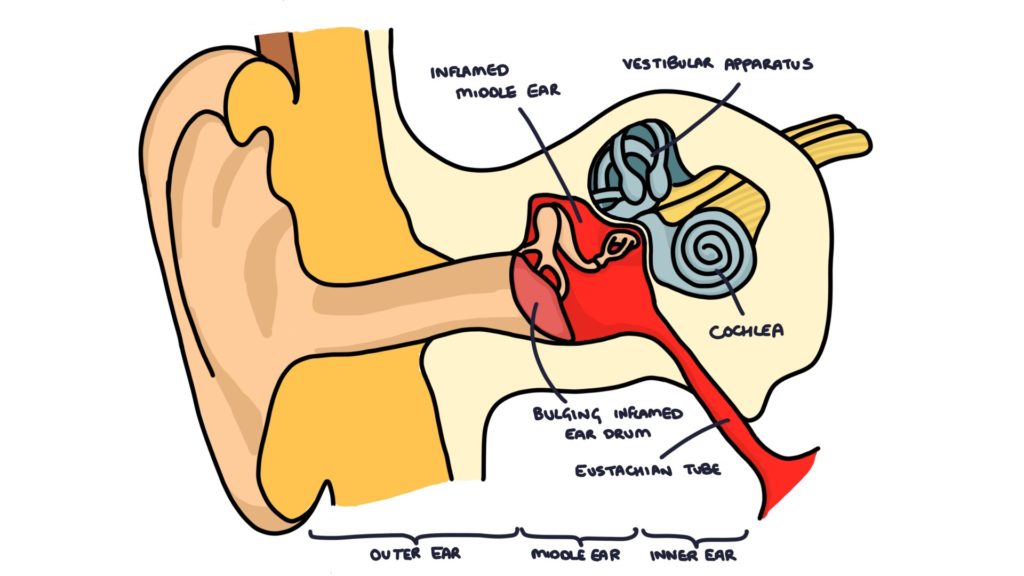
Acute otitis media involves infection in the middle ear.
The middle ear is the air-filled space behind the tympanic membrane. It contains the three auditory ossicles (small bones) and connects to the nasopharynx via the Eustachian tube. It is a very common site of infection in children. Bacteria can enter from the back of the throat through the Eustachian tube.
Causes
Otitis media can be viral or bacterial. The most common bacteria are:
- Streptococcus pneumoniae
- Haemophilus influenzae
- Moraxella catarrhalis
- Streptococcus pyogenes
Presentation
Typical symptoms of otitis media include:
- Ear pain
- Reduced hearing
- Fever
- Ear discharge (if the tympanic membrane is perforated)
Symptoms can be non-specific, particularly in young children and infants. They may present with symptoms such as fever, vomiting, irritability, lethargy, or poor feeding. Parents may notice young children holding or pulling at their ear.
In a well child, the tympanic membrane should be “pearly-grey”, translucent and slightly shiny. The malleus should be visible through the membrane. A cone of light can be seen, reflecting the otoscope’s light.
In otitis media, the tympanic membrane will be bulging, red and inflamed. The malleus and reflection of light are not visible. If the tympanic membrane is perforated, there may be discharge in the ear canal (otorrhoea) and a visible hole in the membrane. It may be difficult to visualise the tympanic membrane if there is significant discharge or wax in the ear canal.
Management
In most cases of otitis media, symptoms resolve within 3 days without antibiotics. Complications are rare. Most cases can be managed with:
- Self-care (e.g., rest and fluids)
- Simple analgesia (e.g., paracetamol or ibuprofen)
- Safety-net advice (e.g., to return if symptoms are worsening or not improving)
Delayed prescriptions can be considered. This involves educating patients or parents that the condition is likely self-limited and does not require antibiotics, but issuing a prescription to be collected if symptoms worsen or do not improve within 3 days.
Immediate or delayed antibiotics may be considered where there is a risk of more significant infection, for example:
- Systemically unwell patients
- Patients with significant co-morbidities
- Children under 2 years with bilateral infection
- Patients with ear discharge (otorrhoea)
The typical antibiotic choices for otitis media are:
- Amoxicillin for 5-7 days
- Clarithromycin or erythromycin in penicillin allergy
- Co-amoxiclav where symptoms are worsening after 2-3 days of amoxicillin
Urgent hospital assessment or admission may be required for:
- Severe systemic infections
- Children at high risk of complications (e.g., immunocompromised)
- Infants under 3 months with a temperature above 38ºC
- Infants under 6 months with a temperature above 39ºC
Complications
- Otitis media with effusion (glue ear)
- Hearing loss (usually temporary)
- Perforated tympanic membrane
- Chronic or recurrent infection
- Mastoiditis (rare)
- Intracranial abscess (rare)
Last updated June 2026
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()