The body goes through a large number of changes during pregnancy. You will come across pregnant women with a high heart rate, low blood pressure, abnormal blood test results and skin changes. It helps to know what changes are normal in healthy pregnant women and when to investigate further for underlying disease.
Hormonal Changes
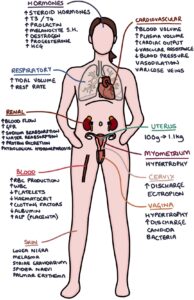
The anterior pituitary gland produces more ACTH, prolactin and melanocyte stimulating hormone in pregnancy.
Higher ACTH levels cause a rise in steroid hormones, particularly cortisol and aldosterone. Higher steroid levels lead to an improvement in most autoimmune conditions and a susceptibility to diabetes and infections.
Increased prolactin acts to suppress FSH and LH, causing reduced FSH and LH levels.
Increased melanocyte stimulating hormone causes increased pigmentation of the skin during pregnancy, resulting in skin changes such as linea nigra and melasma.
TSH remains normal, but T3 and T4 levels rise.
HCG levels rise, roughly doubling every 48 hours until they plateau around 8 – 12 weeks, then gradually start to fall.
Progesterone levels rise throughout pregnancy. Progesterone acts to maintain the pregnancy, prevent contractions and suppress the mother’s immune reaction to fetal antigens. The corpus luteum produces progesterone until ten weeks gestation. The placenta produces it during the remainder of the pregnancy.
Oestrogen rises throughout pregnancy, produced by the placenta.
Changes to the Uterus, Cervix and Vagina
The size of the uterus increases from around 100g to 1.1kg during pregnancy. There is hypertrophy of the myometrium and the blood vessels in the uterus. Increased oestrogen may cause cervical ectropion and increased cervical discharge. Oestrogen also causes hypertrophy of the vaginal muscles and increased vaginal discharge. The changes in the vagina prepare it for delivery, however they make bacterial and candidal infection (thrush) more common.
Before delivery, prostaglandins break down collagen in the cervix, allowing it to dilate and efface during childbirth.
Cardiovascular Changes
There are several cardiovascular changes during pregnancy:
- Increased blood volume
- Increased plasma volume
- Increased cardiac output, with increased stroke volume and heart rate
- Decreased peripheral vascular resistance
- Decreased blood pressure in early and middle pregnancy, returning to normal by term
- Varicose veins can occur due to peripheral vasodilation and obstruction of the inferior vena cava by the uterus
- Peripheral vasodilation also causes flushing and hot sweats
Respiratory Changes
Tidal volume and respiratory rate increase in later pregnancy, to meet the increased oxygen demands.
Renal Changes
A number of changes in the kidneys happen during pregnancy:
- Increased blood flow to the kidneys
- Increased glomerular filtration rate (GFR)
- Increased aldosterone leads to increased salt and water reabsorption and retention
- Increased protein excretion from the kidneys (normal is up to 0.3g in 24 hours)
- Dilatation of the ureters and collecting system, leading to a physiological hydronephrosis (more right-sided)
Haematology and Biochemistry Changes
There is increased red blood cell production in pregnancy, leading to higher iron, folate and B12 requirements. Plasma volume increases more than red blood cell volume, leading to a lower concentration of red blood cells. High plasma volume means the haemoglobin concentration and red cell concentration (haematocrit) fall in pregnancy, resulting in anaemia.
Clotting factors such as fibrinogen and factor VII, VIII and X increase in pregnancy, making women hyper-coagulable. This increases the risk of venous thromboembolism (blood clots developing in the veins). Pregnant women are more likely to develop deep vein thrombosis and pulmonary embolism.
There are a few other changes you may find on blood results:
- Increased white blood cells
- Decreased platelet count
- Increased ESR and D-dimer
- Increased alkaline phosphatase (ALP), up to 4 times normal, due to secretion by the placenta
- Reduced albumin due to loss of proteins in the kidneys
- Calcium requirements increase, but so does gut absorption of calcium, meaning calcium levels remain stable
Skin and Hair Changes
Several changes to skin are normal in pregnancy:
- Increased skin pigmentation due to increased melanocyte stimulating hormone, with linea nigra and melasma
- Striae gravidarum (stretch marks on the expanding abdomen)
- General itchiness (pruritus) can be normal, but can indicate obstetric cholestasis
- Spider naevi
- Palmar erythema
Postpartum hair loss is normal, and usually improves within six months.
Last updated May 2020