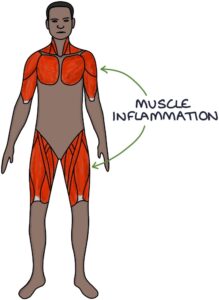
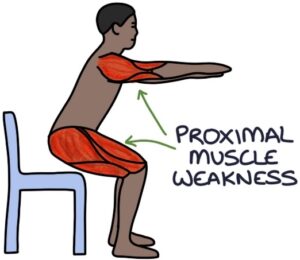
Polymyositis and dermatomyositis are autoimmune disorders causing muscle inflammation (myositis). Both present with proximal muscle weakness.
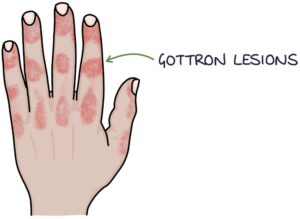
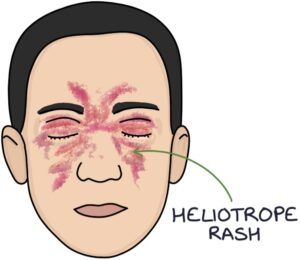
Dermatomyositis also involves characteristic skin changes, specifically Gottron papules affecting the backs of the hands and heliotrope rash affecting the eyelids.
Polymyositis or dermatomyositis can be caused by an underlying cancer, making them paraneoplastic syndromes. A viral infection may be the trigger (e.g., Coxsackie virus or HIV). Certain HLA genes are risk factors.
Presentation
The typical presenting symptom is gradual-onset, symmetrical, proximal muscle weakness, causing difficulties standing from a chair, climbing stairs or lifting overhead. There may be muscle pain (myalgia), but not always.
Polymyositis occurs without any skin features.
Potential skin changes in dermatomyositis include:
- Gottron lesions (scaly erythematous patches) on the knuckles, elbows and knees
- Heliotrope rash (a purple rash on the face and eyelids)
- Periorbital oedema (swelling around the eyes)
- Photosensitive erythematous rash on the back, shoulders and neck
Creatine Kinase
The critical test for myositis is a creatine kinase blood test. Creatine kinase is an enzyme found inside muscle cells. Inflammation in the muscle cells (myositis) releases creatine kinase. Creatine kinase is usually less than about 300 IU/L. With myositis, the result is often in the multiples of thousands.
Other causes of a raised creatine kinase include:
- Rhabdomyolysis
- Acute kidney injury
- Myocardial infarction
- Statins
- Strenuous exercise
Diagnosis
The diagnosis is made by a rheumatology specialist, based on:
- Clinical features
- Elevated creatine kinase
- Autoantibodies
- Electromyography (EMG)
- Magnetic resonance imaging (MRI)
- Muscle biopsy
There are many myositis-specific antibodies with varying associations. The most common one to remember is anti-Jo-1 antibodies associated with polymyositis.
Management
A rheumatologist guides management. New cases are assessed for possible underlying cancer. They may benefit from physiotherapy and occupational therapy to help with muscle strength and function.
Corticosteroids are the first-line treatment of both conditions.
Other medical options where the response to steroids is inadequate:
- Immunosuppressants (e.g., methotrexate or azathioprine)
- IV immunoglobulins
- Biological therapy (e.g., infliximab or etanercept)
Last updated August 2023
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()