Renal tubular acidosis (RTA) involves metabolic acidosis due to pathology in the tubules of the kidneys. The tubules balance hydrogen (H+) and bicarbonate ions (HCO3–) between the blood and urine to maintain a normal pH. There are four types of renal tubular acidosis, with different pathophysiology.
| RTA |
Pathology |
Urinary pH |
Serum Potassium |
| Type 1 |
Distal tubule cannot excrete hydrogen ions |
High |
Low |
| Type 2 |
Proximal tubule cannot reabsorb bicarbonate |
High |
Low |
| Type 4 |
Low aldosterone or impaired aldosterone function |
Low |
High |
TOM TIP: Remembering types 1 and 4 for your exams (type 4 is the most common). Both involve inadequate hydrogen excretion in the distal tubules. In type 1, there is hypokalaemia. In type 4, there is hyperkalaemia.
Type 1 Renal Tubular Acidosis
Type 1 RTA (or distal RTA) occurs when the distal tubule cannot excrete hydrogen ions.
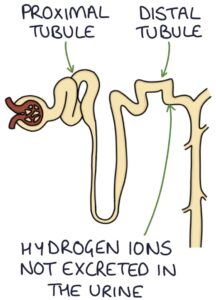
This results in:
- High urinary pH (above 6) due to the absence of hydrogen ions
- Metabolic acidosis, due to retained hydrogen ions in the blood
- Hypokalaemia, due to failure of the hydrogen and potassium exchange (H+/K+ ATPase)
Many conditions can cause this pathology in the distal tubule:
- Genetic (there are both autosomal dominant and autosomal recessive forms)
- Systemic lupus erythematosus
- Sjögren’s syndrome
- Primary biliary cholangitis
- Hyperthyroidism
- Sickle cell anaemia
- Marfan’s syndrome
It presents with:
- Failure to thrive in children
- Recurrent UTIs (due to alkaline urine)
- Bone disease (rickets or osteomalacia)
- Muscle weakness
- Arrhythmias (due to hypokalaemia)
Treatment is with oral bicarbonate, which corrects the acidosis and electrolyte imbalances.
Type 2 Renal Tubular Acidosis
Type 2 RTA (or proximal RTA) occurs when the proximal tubule cannot reabsorb bicarbonate from the urine to the blood, with excessive bicarbonate excreted in the urine.
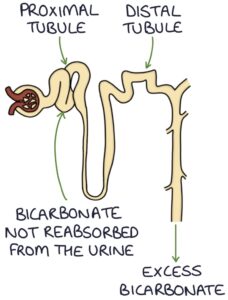
This results in:
- High urinary pH (above 6) due to the excess bicarbonate in the urine
- Metabolic acidosis, due to inadequate bicarbonate in the blood
- Hypokalaemia, due to urinary loss of potassium along with bicarbonate
Key causes are inherited (autosomal dominant or recessive), multiple myeloma and Fanconi’s syndrome.
Treatment is with oral bicarbonate.
Type 3 Renal Tubular Acidosis
Type 3 RTA (or mixed RTA) is a combination of type 1 and 2, with pathology in the proximal and distal tubules. It is rare and unlikely to appear in exams.
Type 4 Renal Tubular Acidosis
Type 4 RTA (or hyperkalaemic RTA) is caused by reduced aldosterone. Aldosterone stimulates sodium reabsorption and potassium and hydrogen ion excretion in the distal tubules. Low aldosterone or impaired aldosterone function leads to insufficient potassium and hydrogen ion excretion.
Normally, ammonia is produced in the distal tubules to balance the excretion of hydrogen ions. Ammonia is a base and buffers the hydrogen ions, preventing the urine from becoming too acidotic. Hyperkalaemia suppresses ammonia production, so the urine becomes acidotic.
The results are:
- Metabolic acidosis, due to retained hydrogen ions in the blood
- Hyperkalaemia, due to retained potassium in the blood
- Low urinary pH due to reduced ammonia production in response to hyperkalaemia
Low aldosterone or low aldosterone activity can be due to:
- Adrenal insufficiency
- Diabetic nephropathy
- Medications (e.g., ACE inhibitors, spironolactone or eplerenone)
Management is targeted at the underlying cause. Fludrocortisone (a mineralocorticoid steroid) may be used in aldosterone deficiency. Oral bicarbonate and treatment of hyperkalaemia may also be required.
Last updated September 2023
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()