Central retinal artery occlusion occurs due to obstruction to blood flow through the central retinal artery. The central retinal artery is a branch of the ophthalmic artery, which is a branch of the internal carotid artery.
The most common cause is atherosclerosis. It can also be caused by giant cell arteritis, where vasculitis affecting the ophthalmic or central retinal artery reduces blood flow.
Risk Factors
Risk factors for cardiovascular disease (e.g., smoking, hypertension, diabetes and raised cholesterol) increase the risk of atherosclerosis causing central retinal artery occlusion.
Risk factors for giant cell arteritis are white ethnicity, older age, female and polymyalgia rheumatica.
Presentation
Blockage of the central retinal artery causes sudden painless loss of vision. It may be described as like a “curtain coming down” over the vision.
There will be a relative afferent pupillary defect, where the pupil in the affected eye constricts more when light is shone in the other eye than when it is shone in the affected eye. The input is not sensed by the ischaemic retina when testing the direct light reflex but is sensed during the consensual light reflex.
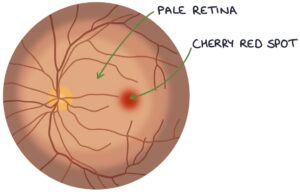
Fundoscopy will show a pale retina with a cherry red spot. The retina is pale due to a lack of perfusion. The cherry red spot is the fovea, which has a thinner surface and shows the red-coloured choroid below.
TOM TIP: The key differentials for a sudden painless vision loss are retinal detachment, central retinal artery occlusion, central retinal vein occlusion or vitreous haemorrhage (due to diabetic retinopathy). Amaurosis fugax describes a temporary loss of vision caused by a temporary interruption to the blood supply.
Management
Central retinal artery occlusion is a vision-threatening emergency. Suspected cases should be referred immediately.
Giant cell arteritis is a potentially reversible cause. Testing includes an ESR blood test and temporal artery biopsy. Treatment is with high-dose systemic steroids.
Immediate management options attempt to dislodge/resolve the blockage. There is no consensus, guidelines or solid evidence base for these options:
- Ocular massage (massaging the eye)
- Anterior chamber paracentesis (removing fluid from the anterior chamber to reduce the intraocular pressure)
- Inhaled carbogen (5% carbon dioxide and 95% oxygen) (to dilate the artery)
- Sublingual isosorbide dinitrate (to dilate the artery)
- Oral pentoxifylline (to dilate the artery)
- Intravenous acetazolamide (to reduce the intraocular pressure)
- Intravenous mannitol (to reduce the intraocular pressure)
- Topical timolol (to reduce the intraocular pressure)
Long-term management involves treating reversible risk factors and secondary prevention of cardiovascular disease.
Last updated October 2023
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()