Epilepsy is a condition characterised by seizures. Seizures are transient episodes of abnormal electrical activity in the brain.
Types of Seizure
The types seen in adults and children include:
- Generalised tonic-clonic seizures
- Focal seizures
- Myoclonic seizures
- Tonic seizures
- Atonic seizures
The types primarily seen in children include:
- Absence seizures
- Infantile spasms
- Febrile convulsions
Generalised tonic-clonic seizures involve tonic (muscle tensing) and clonic (muscle jerking) movements associated with a complete loss of consciousness. Typically, the tonic phase comes before the clonic phase. They are also called grand mal seizures. There may be tongue biting, incontinence, groaning and irregular breathing during the seizure. After the seizure, there is a prolonged postictal period, where the person is confused, tired and irritable or low.
Focal seizures occur in an isolated brain area. They may affect hearing, speech, memory or emotions. Patients remain awake and aware during focal aware seizures (previously simple partial seizures), but lose awareness during focal impaired awareness seizures (previously complex partial seizures). There are various symptoms associated with focal seizures, depending on the location of the abnormal electrical activity, such as:
- Déjà vu
- Strange smells, tastes, vision, or sound sensations
- Unusual emotions
- Abnormal behaviours
Myoclonic seizures present with sudden, brief muscle contractions, like an abrupt jump or jolt. They often remain aware during the seizure. Myoclonic seizures can occur as part of juvenile myoclonic epilepsy in children.
Tonic seizures involve a sudden onset of increased muscle tone, where the entire body stiffens. This results in a fall if the patient is standing, usually backwards. They last only a few seconds, or at most a few minutes.
Atonic seizures (causing “drop attacks”) involve a sudden loss of muscle tone, often resulting in a fall. They last only briefly, and patients are usually aware during the episodes. They often begin in childhood. They may be indicative of Lennox-Gastaut syndrome.
Absence seizures are usually seen in children. The patient becomes blank, stares into space, and then abruptly returns to normal. During the episode, they are unaware of their surroundings and do not respond. These typically last 5 to 15 seconds. Most patients stop having absence seizures as they get older.
Infantile spasms are also known as West syndrome. It is a rare disorder (1 in 4,000) that typically starts around six months of age. It presents with clusters of full-body spasms. Hypsarrhythmia is the characteristic EEG finding. It is associated with developmental regression and has a poor prognosis. Treatment is with:
- High-dose oral prednisolone
- Vigabatrin
Febrile convulsions are tonic-clonic seizures that occur in children during a high fever. They are not caused by epilepsy or other pathology (e.g., meningitis or tumours). Febrile convulsions occur in children aged between 6 months and 5 years. They do not usually cause any lasting damage. One in three will have another febrile convulsion. They slightly increase the risk of developing epilepsy.
Dravet syndrome is an autosomal dominant genetic condition that causes severe epilepsy starting in infancy, typically starting around 6 months. It typically causes prolonged seizures triggered by hot environments or fevers. It can be challenging to treat and is often associated with developmental delay or regression.
Investigations
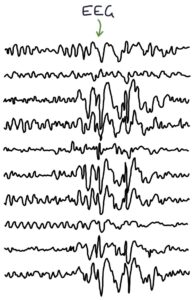
An electroencephalogram (EEG) shows typical patterns in different forms of epilepsy and supports the diagnosis.
MRI brain is used to diagnose structural pathology (e.g., tumours).
Additional investigations can be considered to exclude associated pathology:
- ECG
- Serum electrolytes, including sodium, potassium, calcium and magnesium
- Blood glucose for hypoglycaemia and diabetes
- Blood cultures, urine cultures and lumbar puncture where sepsis, encephalitis or meningitis is suspected
Management
Patients and families presenting with seizures are advised about safety precautions and recognising, managing and reporting further seizures.
Safety precautions include:
- The DVLA will remove their driving licence until specific criteria are met (e.g., being seizure-free for one year)
- Taking showers rather than baths (drowning is a significant risk in epilepsy)
- Particular caution with swimming, heights, traffic and dangerous equipment
Treatment depends on the type of seizure and is guided by a specialist. The aim of treatment is to be seizure-free on the minimum anti-epileptic medications, ideally monotherapy with a single drug. First-line therapies depend on the type of seizure, based on the NICE guidelines (updated 2025):
| Seizure Type | Patients under 55 (male or female) | Patients over 55 |
| Generalised tonic-clonic | Lamotrigine or Levetiracetam | <- or Sodium Valproate |
| Focal | Lamotrigine or Levetiracetam | <- |
| Myoclonic | Levetiracetam | <- or Sodium Valproate |
| Tonic and atonic | Lamotrigine | <- or Sodium Valproate |
| Absence | Ethosuximide | <- |
Other less commonly used anti-epileptic drugs to be aware of include:
- Clobazam
- Carbamazepine
- Phenytoin
- Topiramate
- Gabapentin
- Pregabalin
Sodium Valproate
Sodium valproate increases gamma-aminobutyric acid (GABA) activity, which has a calming effect on the brain. Notable side effects include:
- Teratogenic (harmful in pregnancy)
- Liver damage and hepatitis
- Hair loss
- Tremor
- Reduced fertility
Sodium valproate in pregnancy can cause neural tube defects and developmental delay. There are strict rules for avoiding sodium valproate in females with childbearing potential unless there are no suitable alternatives and strict criteria are met. The Valproate Pregnancy Prevention Programme is in place to ensure this happens, which involves ensuring effective contraception and an annual risk acknowledgement form.
In 2024, the Medicines and Healthcare products Regulatory Agency (MHRA) released drug safety updates regarding the potential increased risk of neurodevelopmental disorders in children fathered by men taking sodium valproate. The MHRA recommended that sodium valproate should not be started in men or women under 55 years of age unless no suitable alternatives are available. Men taking valproate require effective contraception during and for three months after treatment, meaning condoms plus female contraception in their partners.
Status Epilepticus
Status epilepticus is a medical emergency defined as either:
- A seizure lasting more than 5 minutes
- Multiple seizures without regaining consciousness in the interim
Management of status epilepticus involves an ABCDE approach, including:
- Securing the airway
- Giving high-concentration oxygen
- Checking blood glucose levels
- Gaining intravenous access (inserting a cannula)
Medical treatment involves:
- A benzodiazepine first-line, repeated after 5-10 minutes if the seizure continues
- Second-line options (after two doses of benzodiazepine) are IV levetiracetam, phenytoin or sodium valproate
- Third-line options are phenobarbital or general anaesthesia
Options for benzodiazepines are:
- Buccal midazolam (10mg)
- Rectal diazepam (10mg)
- Intravenous lorazepam (4mg)
Last updated January 2026
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()