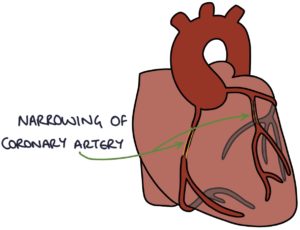
Angina is caused by atherosclerosis affecting the coronary arteries, narrowing the lumen (inside diameter) and reducing blood flow to the myocardium (heart muscle). During times of high demand, such as exercise, there is an insufficient supply of blood to meet the demand. This causes the symptoms of angina, typically constricting chest pain, with or without radiation to the jaw or arms.
Angina is “stable” when symptoms only come on with exertion and are always relieved by rest or glyceryl trinitrate (GTN).
It is “unstable” when the symptoms appear randomly whilst at rest. Unstable angina is a type of acute coronary syndrome (ACS) and requires immediate management.
Investigations
All patients with angina should have the following baseline investigations:
- Physical examination (e.g., heart sounds, signs of heart failure, blood pressure and BMI)
- ECG (a normal ECG does not exclude stable angina)
- FBC (anaemia)
- U&Es (required before starting an ACE inhibitor and other medications)
- LFTs (required before starting statins)
- Lipid profile
- Thyroid function tests (hypothyroidism or hyperthyroidism)
- HbA1C and fasting glucose (diabetes)
Cardiac stress testing involves assessing the patient’s heart function during exertion. This can involve having the patient exercise (e.g., walking on a treadmill) or giving medication (e.g., dobutamine) to stress the heart. The options for assessing cardiac function during stress testing are an ECG, echocardiogram, MRI or a myocardial perfusion scan (nuclear medicine scan).
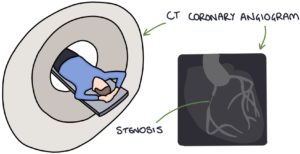
CT coronary angiography involves injecting contrast and taking CT images timed with the heart contractions to give a detailed view of the coronary arteries, highlighting the specific locations of any narrowing.
Invasive coronary angiography involves an invasive procedure performed in a catheter laboratory (cath lab). A catheter is inserted into the patient’s brachial or femoral artery, directed through the arterial system to the aorta and the coronary arteries under x-ray guidance, where contrast is injected to visualise the coronary arteries and identify any areas of stenosis using x-ray images. This is considered the gold standard for determining coronary artery disease.
Management
The management described here is based on NICE clinical knowledge summaries on stable angina (updated August 2022) and chest pain (updated October 2022), and the SIGN guidelines (2018).
There are five principles of management. You can remember this with the “RAMPS” mnemonic:
- R – Refer to cardiology
- A – Advise them about the diagnosis, management and when to call an ambulance
- M – Medical treatment
- P – Procedural or surgical interventions
- S – Secondary prevention
Referrals are usually sent to the rapid access chest pain clinic (RACPC).
Medical Management
There are three aims of medical management:
- Immediate symptomatic relief during episodes of angina
- Long-term symptomatic relief
- Secondary prevention of cardiovascular disease
Immediate symptomatic relief is with sublingual glyceryl trinitrate (GTN) in the form of a spray or tablets. GTN causes vasodilation, improving blood flow to the heart muscle (myocardium). Patients are advised to:
- Take the GTN when the symptoms start
- Take a second dose after 5 minutes if the symptoms remain
- Call an ambulance if the symptoms remain 5 minutes after the second dose
Key side effects of GTN are headaches and dizziness caused by vasodilation.
For long-term symptomatic relief, first-line is with either, or a combination, of:
- Beta blocker (e.g., bisoprolol)
- Calcium-channel blocker (e.g., diltiazem or verapamil – both avoided in heart failure with reduced ejection fraction)
A specialist may consider other options for long-term symptomatic relief:
- Long-acting nitrates (e.g., isosorbide mononitrate)
- Ivabradine
- Nicorandil
- Ranolazine
Medications for secondary prevention can be remembered with the “four As” mnemonic:
- A – Aspirin 75mg once daily
- A – Atorvastatin 80mg once daily
- A – ACE inhibitor (if diabetes, hypertension, CKD or heart failure are also present)
- A – Already on a beta blocker for symptomatic relief
Surgical Interventions
Surgical procedures are generally offered to patients with more severe disease and where medical treatments do not control symptoms. There are two options:
- Percutaneous coronary intervention (PCI)
- Coronary artery bypass graft (CABG)
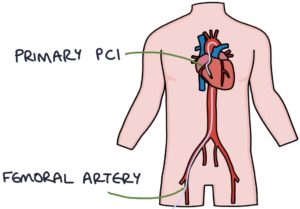
Percutaneous coronary intervention (PCI) involves inserting a catheter into the patient’s brachial or femoral artery. This is fed in, under x-ray guidance, through the arterial system to the coronary arteries. Then a contrast is injected to visualise the coronary arteries and identify areas of stenosis on the x-ray images. Areas of stenosis can be treated by dilating a balloon to widen the lumen (angioplasty) and inserting a stent to keep it open. This can be referred to as coronary angioplasty and stenting.
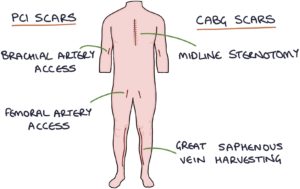
Coronary artery bypass graft (CABG) surgery may be offered to patients with severe stenosis. This involves opening the chest along the sternum, with a midline sternotomy incision. A graft vessel is attached to the affected coronary artery, bypassing the stenotic area. The three main options for graft vessels are:
- Saphenous vein (harvested from the inner leg)
- Internal thoracic artery, also known as the internal mammary artery
- Radial artery

Generally, short and medium-term outcomes are similar between PCI and CABG. However, PCI has a:
- Faster recovery
- Lower rate of strokes as a complication
- Higher rate of requiring repeat revascularisation (further procedures)
TOM TIP: When examining a patient that you think may have coronary artery disease in your OSCEs, check for a midline sternotomy scar (previous CABG), scars around the brachial and femoral arteries (previous PCI) and along the inner calves (saphenous vein harvesting scar) to see what procedures they may have had done.
Cardiac Syndrome X
Cardiac syndrome X causes angina-like chest pain without the presence of coronary artery disease when investigated with angiograms. It occurs most commonly in women in the perimenopausal or postmenopausal period (aged 45 – 55).
The pathophysiology is not fully understood. It may involve microvascular dysfunction, causing reduced blood flow. It may also be due to increased sensitivity of the heart muscle (myocardium), lowering the pain threshold.
Cardiac syndrome X is a diagnosis of exclusion. Patients are fully investigated to exclude coronary artery disease and other pathology. Treatment options for symptoms are similar to the medical management of angina.
Last updated March 2023
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()