Pacemakers deliver controlled electrical impulses to specific areas of the heart to improve heart function. They consist of a pulse generator (the pacemaker box) and the pacing leads, which carry electrical impulses to the relevant part of the heart. The box is implanted under the skin (most commonly in the left anterior chest wall). The wires fed into the left subclavian vein and through the venous system to the relevant chambers of the heart.
Patients with a pacemaker are followed up regularly to download information from the pacemaker, check everything is working ok, and decide when the battery needs replacing. They are given an identity card and bracelet.
Pacemakers do not interact with most day-to-day electrical activities. However, they may be incompatible with MRI scans (due to powerful magnets), TENS machines (used for pain management) and diathermy (used during surgical procedures). Many modern pacemakers are MRI-compatible. Some smartphones may interact with pacemakers if held too close. Devices with strong magnets (e.g., handheld security scanners at airports) can affect the pacemaker function.
TOM TIP: Pacemakers must be removed before cremation in deceased patients. On the cremation form, one of the most critical tasks is to confirm whether the body has a pacemaker and whether it has been removed. You may hear stories about pacemakers “blowing up” crematoriums (this is a dramatic exaggeration, but they can explode, causing significant damage).
Indications
Indications for a pacemaker include:
- Symptomatic bradycardias (e.g., due to sick sinus syndrome)
- Mobitz type 2 heart block
- Third-degree heart block
- Atrioventricular node ablation for atrial fibrillation
- Severe heart failure (biventricular pacemakers)
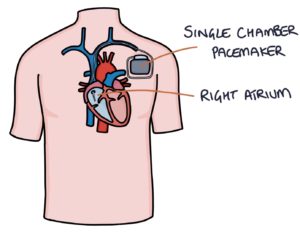
Single-chamber
Single-chamber pacemakers have leads in a single chamber, either the right atrium or the right ventricle.
They are placed in the right atrium if the issue is with the sinoatrial node and conduction through the atrioventricular node is normal. This way, they stimulate depolarisation in the right atrium, and this electrical activity passes to the left atrium and ventricles.
They are placed in the right ventricle if conduction through the atrioventricular node is abnormal. They stimulate the ventricles directly.
Dual-chamber
Dual-chamber pacemakers have leads in both the right atrium and right ventricle. The pacemaker coordinates the contraction of the atria and ventricles.

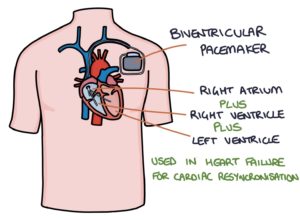
Biventricular (Triple-Chamber) Pacemaker
Biventricular pacemakers have leads in the right atrium, right ventricle and left ventricle.
They are usually in patients with severe heart failure. They coordinate the contraction of these chambers to optimise heart function. This is referred to as cardiac resynchronisation therapy (CRT).
Implantable Cardioverter Defibrillators
Implantable cardioverter defibrillators (ICDs) continually monitor the heart and apply a defibrillator shock if they identify ventricular tachycardia or ventricular fibrillation.
Implantable cardioverter defibrillators are used in patients at risk of ventricular tachycardia or fibrillation, for example:
- Previous cardiac arrest
- Hypertrophic obstructive cardiomyopathy
- Long QT syndrome
ECG Changes
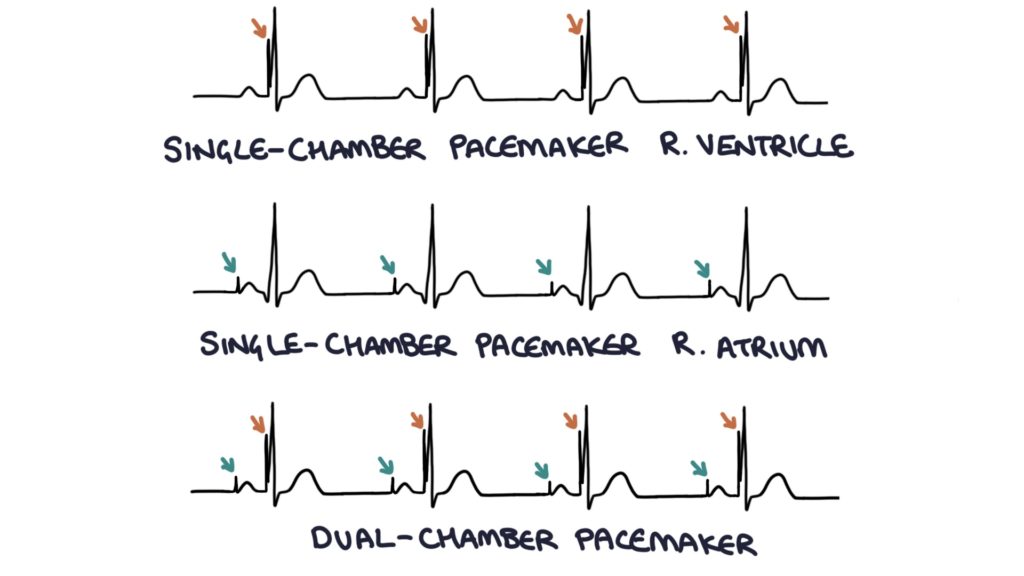
The pacemaker intervention can be seen as a sharp vertical line on all leads on the ECG trace. A line before each P wave indicates a lead in the atria. A line before each QRS complex indicates a lead in the ventricles. Therefore:
- A line before either the P wave or QRS complex but not the other indicates a single-chamber pacemaker
- A line before both the P wave and QRS complex indicates a dual-chamber pacemaker
TOM TIP: It is worth ensuring you can identify the type of pacemaker on an ECG, as this is common in exams.
Last updated March 2023
Now, head over to members.zerotofinals.com and test your knowledge of this content. Testing yourself helps identify what you missed and strengthens your understanding and retention.
![]()