Fibroids are benign tumours of the smooth muscle of the uterus. They are also called uterine leiomyomas. They are very common, affecting 40-60% of women in later reproductive years, and are more common in black women compared with other ethnic groups. They are oestrogen sensitive, meaning they grow in response to oestrogen.
Types
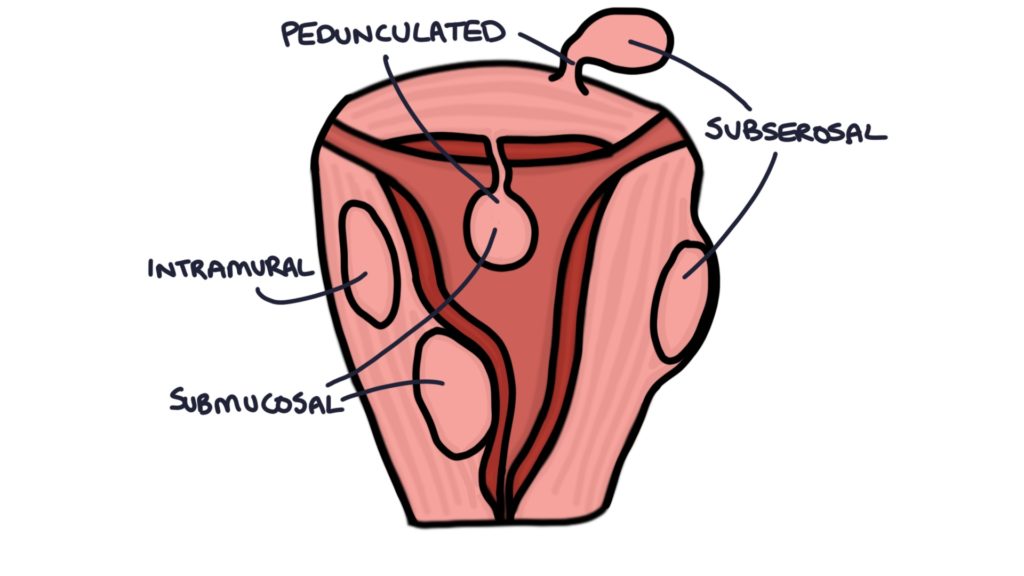
- Intramural means within the myometrium (the muscle of the uterus). As they grow, they change the shape and distort the uterus.
- Subserosal means just below the outer layer of the uterus. These fibroids grow outwards and can become very large, filling the abdominal cavity.
- Submucosal means just below the lining of the uterus (the endometrium).
- Pedunculated means on a stalk.
Presentation
Fibroids are often asymptomatic. They can present in several ways:
- Heavy menstrual bleeding (menorrhagia) is the most frequent presenting symptom
- Prolonged menstruation, lasting more than 7 days
- Abdominal pain, worse during menstruation
- Bloating or feeling full in the abdomen
- Urinary or bowel symptoms due to pelvic pressure or fullness
- Deep dyspareunia (pain during intercourse)
- Reduced fertility
Abdominal and bimanual examination may reveal a palpable pelvic mass or an enlarged firm non-tender uterus.
Investigations
Hysteroscopy is the initial investigation for submucosal fibroids presenting with heavy menstrual bleeding.
Pelvic ultrasound is the investigation of choice for larger fibroids.
MRI scanning may be considered before surgical options, where more information is needed about the size, shape and blood supply of the fibroids.
Management
NICE guidelines on fibroids are included within the heavy menstrual bleeding guideline from 2018.
For fibroids less than 3 cm, the medical management is the same as with heavy menstrual bleeding:
- Mirena coil (1st line) – fibroids must be less than 3cm with no distortion of the uterus
- Symptomatic management with NSAIDs and tranexamic acid
- Combined oral contraceptive
- Cyclical oral progestogens
Surgical options for managing smaller fibroids with heavy menstrual bleeding are:
- Endometrial ablation
- Resection of submucosal fibroids during hysteroscopy
- Hysterectomy
For fibroids more than 3 cm, women need referral to gynaecology for investigation and management. Medical management options are:
- Symptomatic management with NSAIDs and tranexamic acid
- Mirena coil – depending on the size and shape of the fibroids and uterus
- Combined oral contraceptive
- Cyclical oral progestogens
Surgical options for larger fibroids are:
- Uterine artery embolisation
- Myomectomy
- Hysterectomy
GnRH agonists, such as goserelin (Zoladex) or leuprorelin (Prostap), may be used to reduce the size of fibroids before surgery. They work by inducing a menopause-like state and reducing the amount of oestrogen maintaining the fibroid. Usually, GnRH agonists are only used short term, for example, to shrink a fibroid before myomectomy.
Uterine Artery Embolisation
Uterine artery embolisation is a surgical option for larger fibroids, performed by interventional radiologists. The radiologist inserts a catheter into an artery, usually the femoral artery. This catheter is passed through to the uterine artery under X-ray guidance. Once in the correct place, particles are injected that cause a blockage in the arterial supply to the fibroid. This starves the fibroid of oxygen and causes it to shrink.
Surgical Options
Myomectomy involves surgically removing the fibroid via laparoscopic (keyhole) surgery or laparotomy (open surgery). Myomectomy is the only treatment known to potentially improve fertility in patients with fibroids.
Endometrial ablation can be used to destroy the endometrium. Second generation, non-hysteroscopic techniques are used, such as balloon thermal ablation. This involves inserting a specially designed balloon into the endometrial cavity and filling it with high-temperature fluid that burns the endometrial lining of the uterus.
Hysterectomy involves removing the uterus and fibroids. Hysterectomy may be by laparoscopy (keyhole surgery), laparotomy or vaginal approach. The ovaries may be removed or left depending on patient preference, risks and benefits.
Complications
There are several potential complications of fibroids:
- Heavy menstrual bleeding, often with iron deficiency anaemia
- Reduced fertility
- Pregnancy complications, such as miscarriages, premature labour and obstructive delivery
- Constipation
- Urinary outflow obstruction and urinary tract infections
- Red degeneration of the fibroid
- Torsion of the fibroid, usually affecting pedunculated fibroids
- Malignant change to a leiomyosarcoma is very rare (<1%)
Red Degeneration of Fibroids
Red degeneration refers to ischaemia, infarction and necrosis of the fibroid due to disrupted blood supply. Red degeneration is more likely to occur in larger fibroids (above 5 cm) during the second and third trimester of pregnancy. Red degeneration may occur as the fibroid rapidly enlarges during pregnancy, outgrowing its blood supply and becoming ischaemic. It may also occur due to kinking in the blood vessels as the uterus changes shape and expands during pregnancy.
Red degeneration presents with severe abdominal pain, low-grade fever, tachycardia and often vomiting. Management is supportive, with rest, fluids and analgesia.
TOM TIP: Look out for the pregnant woman with a history of fibroids presenting with severe abdominal pain and a low-grade fever in your exams. The diagnosis is likely to be red degeneration.
Last updated June 2020