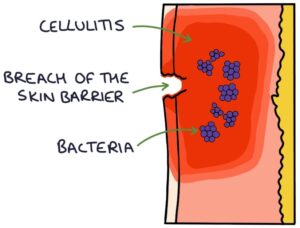
Cellulitis is an infection of the skin and the soft tissues underneath. The skin forms a physical barrier between the environment and soft tissues. When a patient presents with cellulitis, look for a breach in the skin barrier and a point of entry for the bacteria. This may be due to skin trauma, eczema, fungal nail infections or ulcers.
Presentation
Skin changes in cellulitis include:
- Erythema (red discolouration)
- Warm or hot to touch
- Tense
- Thickened
- Oedematous
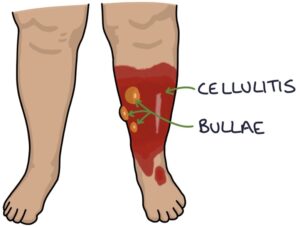
- Bullae (fluid-filled blisters)
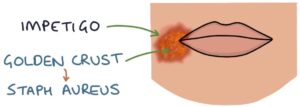
- A golden-yellow crust indicates a Staphylococcus aureus infection
Patients may be systemically unwell, including having sepsis.
Causes
The most common causes are:
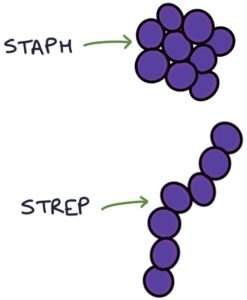
- Staphylococcus aureus
- Group A streptococcus (mainly streptococcus pyogenes)
- Group C streptococcus (mainly streptococcus dysgalactiae)
MRSA should be considered, particularly in patients the repeated hospital admissions and antibiotics.
Eron Classification
The Eron classification assesses the severity of cellulitis:
- Class 1 – no systemic toxicity or comorbidity
- Class 2 – systemic toxicity or comorbidity
- Class 3 – significant systemic toxicity or significant comorbidity
- Class 4 – sepsis or life-threatening infection
Management
Class 3 and 4 cellulitis requires admission for intravenous antibiotics. Admission is also considered for frail, very young or immunocompromised patients and those with facial, periorbital or orbital cellulitis.
Flucloxacillin is the usual first-line antibiotic for cellulitis, either oral or intravenous. It is particularly effective against Staphylococcus aureus and also works well against other gram-positive cocci.
Alternatives:
- Clarithromycin
- Clindamycin
- Co-amoxiclav (the usual first choice for cellulitis near the eyes or nose)
Last updated July 2023