Gout is a type of crystal arthropathy associated with chronically high blood uric acid levels. Urate crystals are deposited in the joint, causing it to become inflamed. Gout typically presents with a single acute hot, swollen and painful joint. The critical differential diagnosis for this presentation is septic arthritis.
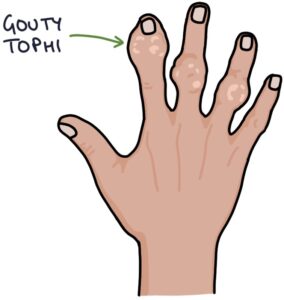
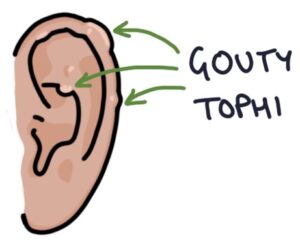
Gouty tophi are subcutaneous uric acid deposits typically seen on the hands, elbows and ears.

Risk Factors
- Male
- Family history
- Obesity
- High purine diet (e.g., meat and seafood)
- Alcohol
- Diuretics
- Cardiovascular disease
- Kidney disease
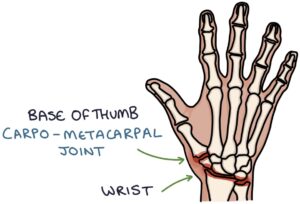
Typical Joints
The most commonly affected joints are:
- The base of the big toe – the metatarsophalangeal joint (MTP joint)
- The base of the thumb – the carpometacarpal joint (CMC joint)
- Wrist

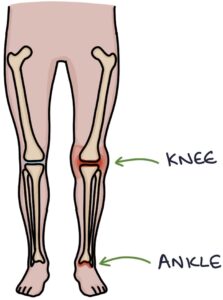
Gout can also affect larger joints (e.g., knee and ankle).
Diagnosis
Diagnosis is usually made clinically, supported by a raised serum urate level on a blood test.
It is essential to exclude septic arthritis, a potentially life-threatening differential diagnosis. Any suspicion of septic arthritis requires emergency management with joint aspiration and antibiotics.
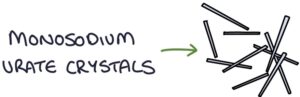
Aspirated joint fluid shows monosodium urate crystals. These are needle-shaped and negatively birefringent of polarised light. There should be no bacterial growth.
TOM TIP: A common exam question asks you to diagnose gout or pseudogout using joint fluid examination. The monosodium urate crystals of gout are needle-shaped and negatively birefringent of polarised light. The calcium pyrophosphate crystals of pseudogout are rhomboid-shaped and positively birefringent.
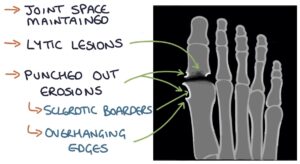
X-ray of a joint affected by gout shows:
- Maintained joint space (no loss of joint space)
- Lytic lesions in the bone
- Punched out erosions
- Erosions can have sclerotic borders with overhanding edges
Management
Acute flares are treated with:
- NSAIDs (e.g., naproxen) first-line (co-prescribed with a proton pump inhibitor for gastroprotection)
- Colchicine second-line
- Oral steroids (e.g., prednisolone) third-line
Colchicine is used in patients who are inappropriate for NSAIDs, such as those with renal impairment or significant heart disease. Abdominal symptoms and diarrhoea are common side effects. These may be mild and resolve with a reduced dose. However, more severe symptoms may indicate toxicity. Colchicine is very dangerous in overdose and can cause multiple organ failure. It is only prescribed for a short course (up to 6mg per course).
Prophylaxis is with xanthine oxidase inhibitors, which lower the uric acid level. The options are:
- Allopurinol
- Febuxostat
Lifestyle changes can reduce the risk of gout. This involves losing weight, staying hydrated and minimising the consumption of alcohol and purine-based food (e.g., meat and seafood).
TOM TIP: Prophylaxis is not started until weeks after the acute attack has resolved. NSAIDs or colchicine may be given to prevent a gout attack during the initial period. Once allopurinol or febuxostat is initiated, it is continued during an acute attack. These facts are commonly tested in exams.
Last updated August 2023