Hyperkalaemia refers to a raised serum potassium. The main complication of hyperkalaemia is cardiac arrhythmias, such as ventricular fibrillation, which can lead to cardiac arrest.
|
Serum Potassium (mmol/L) |
|
|
Normal |
3.5 – 5.3 |
|
Mild Hyperkalaemia |
5.4 – 6 |
|
Moderate Hyperkalaemia |
6 – 6.5 |
|
Severe Hyperkalaemia |
Over 6.5 |
Causes
Conditions that can cause hyperkalaemia include:
- Acute kidney injury
- Chronic kidney disease (stage 4 or 5)
- Rhabdomyolysis
- Adrenal insufficiency
- Tumour lysis syndrome
Medications that can cause hyperkalaemia include:
- Aldosterone antagonists (e.g., spironolactone and eplerenone)
- ACE inhibitors (e.g., ramipril)
- Angiotensin II receptor blockers (e.g., candesartan)
- NSAIDs (e.g., naproxen)
Haemolysis (rupture of blood cells) during sampling can create a falsely elevated potassium (pseudohyperkalaemia). The lab might indicate that they have noticed some haemolysis and recommend a repeat sample.
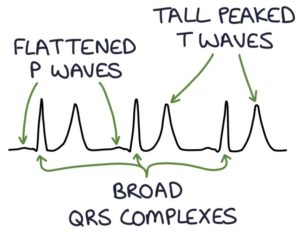
ECG Changes
- Tall peaked T-waves
- Flattening or absence of P waves
- Prolonged PR interval
- Broad QRS complexes
Management
Each hospital will have a policy and protocol to follow for hyperkalaemia. There should be input from experienced seniors, including the intensive care team for severe hyperkalaemia and renal physicians for renal impairment.
Management of serum potassium below 6.5 mmol/L without ECG changes is aimed at the underlying cause, for example, treating acute kidney injury and stopping medications (e.g., spironolactone or ACE inhibitors).
Patients require urgent treatment for hyperkalaemia if they have either:
- ECG changes
- Serum potassium above 6.5 mmol/L
The mainstay of treatment is with an insulin and dextrose infusion and IV calcium gluconate:
- Insulin drives potassium from the extracellular space to the intracellular space
- Dextrose is required to prevent hypoglycaemia while on insulin
- Calcium gluconate stabilises the cardiac muscle cells and reduces the risk of arrhythmias
Other options for lowering the serum potassium are:
- Nebulised salbutamol temporarily drives potassium into cells
- Oral calcium resonium reduces potassium absorption in the GI tract (this is slow and causes constipation)
- Sodium bicarbonate (in acidotic patients on renal advice) drives potassium into cells as it corrects the acidosis
- Haemodialysis may be required in severe or persistent cases
Last updated September 2023