The pupil is formed by a hole in the centre of the iris. Many conditions that cause abnormally shaped or sized pupils.
Pupil Size
The circular muscles in the iris are responsible for pupil constriction. They are stimulated by the parasympathetic nervous system using acetylcholine as a neurotransmitter. The parasympathetic fibres travel along the oculomotor nerve (cranial nerve III).
The dilator muscles in the iris are responsible for pupil dilation. They are arranged like spokes on a bicycle wheel, travelling straight from the inside to the outside of the iris. They are stimulated by the sympathetic nervous system, using adrenalin as a neurotransmitter.
TOM TIP: I picture a parrot sitting on the arch of the circular muscles to remember that the parasympathetic nervous system innervates these muscles and controls pupil constriction.
Abnormal Pupil Shape
Trauma to the sphincter muscles in the iris can cause an irregular pupil shape (e.g., during cataract surgery).
Anterior uveitis can cause adhesions (scar tissue) in the iris, causing an irregular pupil shape.
Acute angle-closure glaucoma can cause ischaemic damage to the muscles of the iris and an abnormal pupil shape, usually a vertical oval.
Rubeosis iridis (neovascularisation in the iris) can distort the shape of the iris and pupil. This is usually associated with poorly controlled diabetes and diabetic retinopathy.
Coloboma is a congenital malformation that can cause a hole in the iris and an irregular pupil shape.
Tadpole pupil involves muscle spasm in part of the dilator muscle of the iris, causing a misshapen pupil. It is a temporary condition and may be associated with migraines and Horner syndrome.
Causes of Mydriasis (Dilated Pupil)
- Congenital
- Stimulants (e.g., cocaine)
- Anticholinergics (e.g., oxybutynin)
- Trauma
- Third nerve palsy
- Holmes-Adie syndrome
- Raised intracranial pressure
- Acute angle-closure glaucoma
Causes of Miosis (Constricted Pupil)
- Horner syndrome
- Cluster headaches
- Argyll-Robertson pupil (neurosyphilis)
- Opiates
- Nicotine
- Pilocarpine
Third Nerve Palsy
A palsy in the third cranial nerve (the oculomotor nerve) causes:
- Ptosis (drooping upper eyelid)
- Dilated non-reactive pupil
- Divergent strabismus (squint) in the affected eye, with a “down and out” position of the affected eye
The third cranial nerve is the oculomotor nerve. It supplies all the extraocular muscles except the lateral rectus and superior oblique. Therefore, when the oculomotor nerve stops working, most of the extraocular muscles stop working, and the lateral rectus and superior oblique (which are still working) pull the eye downward and outward.
The oculomotor nerve also supplies the levator palpebrae superioris, which is responsible for lifting the upper eyelid. Therefore, a third nerve palsy causes ptosis (drooping of the upper eyelid).
The oculomotor nerve carries parasympathetic fibres that innervate the circular muscles of the iris. Therefore, third nerve palsy causes a dilated, non-reactive pupil.
Third nerve palsy can be idiopathic, without a clear cause.
A third nerve palsy that does not affect the pupil (sparing of the pupil) suggests a microvascular cause, as the parasympathetic fibres are spared. This may be due to:
- Diabetes
- Hypertension
- Ischaemia
A full third nerve palsy is caused by compression of the nerve, including compression of the parasympathetic fibres. This may be due to:
- Tumour
- Trauma
- Cavernous sinus thrombosis
- Posterior communicating artery aneurysm
- Raised intracranial pressure
The oculomotor nerve travels directly from the brainstem to the eye in a straight line. It travels through the cavernous sinus and close to the posterior communicating artery. Therefore, cavernous sinus thrombosis or a posterior communicating artery aneurysm can cause nerve compression.
Horner Syndrome
Horner syndrome involves a triad of:
- Ptosis
- Miosis
- Anhidrosis (loss of sweating)
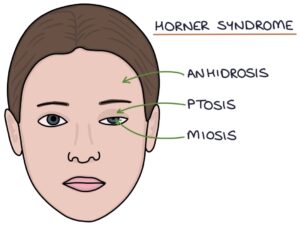
There may also be enopthalmos, which is a sunken eye. Light and accommodation reflexes are not affected.
Horner syndrome is caused by damage to the sympathetic nervous system supplying the face.
The sympathetic nerves arise from the spinal cord in the chest. These are pre-ganglionic nerves. They enter the sympathetic ganglion at the base of the neck and exit as post-ganglionic nerves. The post-ganglionic nerves travel to the head alongside the internal carotid artery.
The location of the Horner syndrome can be determined by the anhidrosis (loss of sweating). Central lesions (occurring before the nerves exit the spinal cord) cause anhidrosis of the arm, trunk and face. Pre-ganglionic lesions cause anhidrosis of the face. Post-ganglionic lesions do not cause anhidrosis.
The causes can be remembered as the 4 Ss, 4 Ts and 4 Cs mnemonic. S for Sentral, T for Torso (pre-ganglionic) and C for Cervical (post-ganglionic).
Central lesions:
- S – Stroke
- S – Multiple Sclerosis
- S – Swelling (tumours)
- S – Syringomyelia (cyst in the spinal cord)
Pre-ganglionic lesions:
- T – Tumour (Pancoast tumour)
- T – Trauma
- T – Thyroidectomy
- T – Top rib (a cervical rib growing above the first rib and clavicle)
Post-ganglionic lesions:
- C – Carotid aneurysm
- C – Carotid artery dissection
- C – Cavernous sinus thrombosis
- C – Cluster headache
Congenital Horner syndrome is associated with heterochromia (a difference in iris colour on the affected side).
Cocaine eye drops can be used to test for Horner syndrome. It acts on the eye to stop noradrenalin re-uptake at the neuromuscular junction. This causes a normal eye to dilate as noradrenalin stimulates the dilator muscles of the iris. In Horner syndrome, the nerves are not releasing noradrenalin, so blocking re-uptake makes no difference, and there is no pupil reaction.
Alternatively, low-dose adrenalin eye drops (0.1%) will dilate the pupil in Horner syndrome but not a normal pupil.
Holmes-Adie Pupil
A Holmes-Adie pupil is caused by damage to the post-ganglionic parasympathetic fibres. The cause is unknown. A Holme-Adie pupil is:
- Dilated
- Sluggish to react to light
- Responsive to accommodation (the pupils constrict well when focusing on a near object)
- Slow to dilate following constriction (“tonic” pupil)
Holmes-Adie syndrome features a Holmes-Adie pupil with absent ankle and knee reflexes.
Argyll-Robertson Pupil
An Argyll-Robertson pupil is a specific finding in neurosyphilis. It is a constricted pupil that accommodates when focusing on a near object but does not react to light. They are often irregularly shaped. It is commonly called a “prostitute’s pupil” due to its relation to neurosyphilis and because “it accommodates but does not react”.
Last updated October 2023