Wilson’s disease is an autosomal recessive genetic condition resulting in the excessive accumulation of copper in the body tissues, particularly in the liver.
It is caused by mutations in the Wilson disease protein gene on chromosome 13 (also called the ATP7B copper-binding protein). This copper-transporting protein is important in helping remove excess copper from the body via the liver. Copper is excreted in the bile.
Features
Wilson’s disease typically presents in teenagers or young adults. It is rare for symptoms to start after age 40. The presenting features vary significantly between individuals. Liver problems usually arise first. Rarely it can present initially with neurological or psychiatric problems, although these typically occur with more advanced disease.
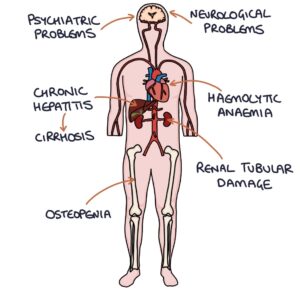
Copper deposition in the liver leads to chronic hepatitis, eventually leading to cirrhosis. Copper deposition in the central nervous system can lead to neurological and psychiatric problems.
Neurological symptoms can include tremor, dysarthria (speech difficulties) and dystonia (abnormal muscle tone). Copper deposition in the basal ganglia causes Parkinsonism (tremor, bradykinesia and rigidity).
Psychiatric symptoms can include abnormal behaviour, depression, cognitive impairment and psychosis.
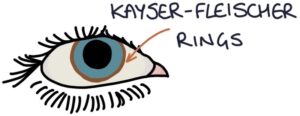
Kayser-Fleischer rings in the cornea (deposition of copper in Descemet’s membrane) may be seen in Wilson’s disease. These are green-brown circles surrounding the iris of the eye. They can usually be seen by the naked eye but proper assessment is made using slit lamp examination.
Haemolytic anaemia (low haemoglobin caused by red blood cell destruction) may also be a feature.
Diagnosis
Serum caeruloplasmin is the initial screening test for suspected Wilson’s disease. A low serum caeruloplasmin is suggestive of Wilson’s disease. Caeruloplasmin is the protein that carries copper in the blood. It can be falsely normal or elevated in cancer or inflammatory conditions.
A 24-hour urine copper assay will show high urinary copper.
Liver biopsy can be used to assess the liver copper content and assess liver disease.
Scoring systems that consider various features and laboratory results are used to establish the diagnosis.
Other investigations:
- Kayser-Fleischer rings on slit lamp examination
- MRI brain may show changes, including the characteristic “double panda sign”
- Low haemoglobin with haemolytic anaemia (negative Coombs test)
- Genetic testing (including screening family members)
Management
Treatment is with copper chelation using either:
- Penicillamine
- Trientine
Other treatments include:
- Zinc salts (inhibit copper absorption in the gastrointestinal tract)
- Liver transplantation
Last updated May 2023